

LifeSpace
Creating a personalized interactive experience that motivates older adults to stay active and healthy
Project type: Final Degree Project (Biomedical Engineering, UPM)
Role: UX/UI Designer
Timeframe: 4 months
Tool: Figma – Dual Prototype (Samsung Flip & Mobile)
Problem
As people age, they often experience a gradual decline in physical and cognitive health, reducing their quality of life and independence
Challenges
1/ Older adults tend to become aware of their health only when problems arise, rather than actively practicing self-care
2/ The adoption of digital technologies among elderly remains low
Goal
Design a personalized experience that encourages active and healthy aging and test it in a Living Lab environment
Research
Back in 2020, when this project was carried out, AI was not yet embedded in our daily lives the way it is today. The research relied mainly on deep desk research and valuable conversations with fellow researchers experienced in working with older adults and Living Labs.
From there, I conducted a state-of-the-art analysis covering digital health, eHealth, and technological solutions for aging and chronic disease management
The analysis revealed a gap: most solutions were either too clinical or fail to offer engaging, holistic interactions that truly empower older adults.
KEY INSIGHTS
-
The demographic shift
Projections highlight the dramatic increase of the elderly population, with direct implications for healthcare systems.
-
Chronic disease and care models
Longer life expectancy correlates with the rising incidence of chronic conditions, requiring new models of care that shift the focus “from disease to patient,” prioritizing prevention, self-care, and holistic well-being.
-
Digital transformation in healthcare
The COVID-19 pandemic accelerated the adoption of telemedicine, electronic health records, and connected devices, yet regulatory frameworks often lag behind innovation.
-
EU initiatives as reference points
Programs such as the EIP on AHA and other European projects were taken as benchmarks for promoting physical and cognitive well-being in older adults.
WHERE DO LIVING LABS COME IN?
- Originating at MIT in 2003, the Living Lab concept quickly expanded worldwide as a collaborative innovation framework.
- In Europe, the ENoLL (European Network of Living Labs) and later the EIT Health Living Labs & Test Beds Network fostered specialized labs in health and AHA, with UPM and LifeSTech playing a leading role in their early development.
- Living Labs apply co-creation and co-design methodologies to involve users throughout the entire lifecycle of a solution, from ideation to validation.
The project was carried out in the Smart House Living Lab (UPM), a 150 m² accessible, sensor-equipped environment simulating a real home. Its versatility makes it an ideal ecosystem for experimenting with digital health technologies in contexts tailored to older adults and people with disabilities.


Empathize
I mapped the four main profiles visiting the Smart House Living Lab:




Profile
Interests
Experience Goals
Maintaining health and independence; exploring innovative solutions to support clinical conditions (e.g., cognitive decline, Parkinson’s, frailty).
Provide a personalized, hands-on experience that aligns with individual needs and preferences, allowing them to directly interact with digital health technologies that foster independent living.
Discovering and testing innovative health solutions; integrating technologies into daily practice; identifying opportunities for collaboration in research and innovation.
Offer a tailored journey through tools (apps, dashboards, web solutions) that supports their professional activities and assists in decision-making.
Exploring cutting-edge innovations in AHA, healthcare, smart cities, ICT, and pharma; evaluating opportunities for co-creation, validation, and scalability; identifying potential business or consulting partnerships.
Present clear insights into existing solutions to evaluate collaboration opportunities, either through private contracts, agreements, or integration into the LifeSTech ecosystem.
Learning about real-world applications of emerging technologies; exploring opportunities in health, AHA, ICT, and smart environments; seeking academic pathways (TFGs, PhDs, projects).
Deliver an interactive experience that highlights opportunities to collaborate with LifeSTech, pursue academic projects, or engage in joint research initiatives.
From these groups, I focused on Older Adults as the primary target. They were stratified according to established dimensions:
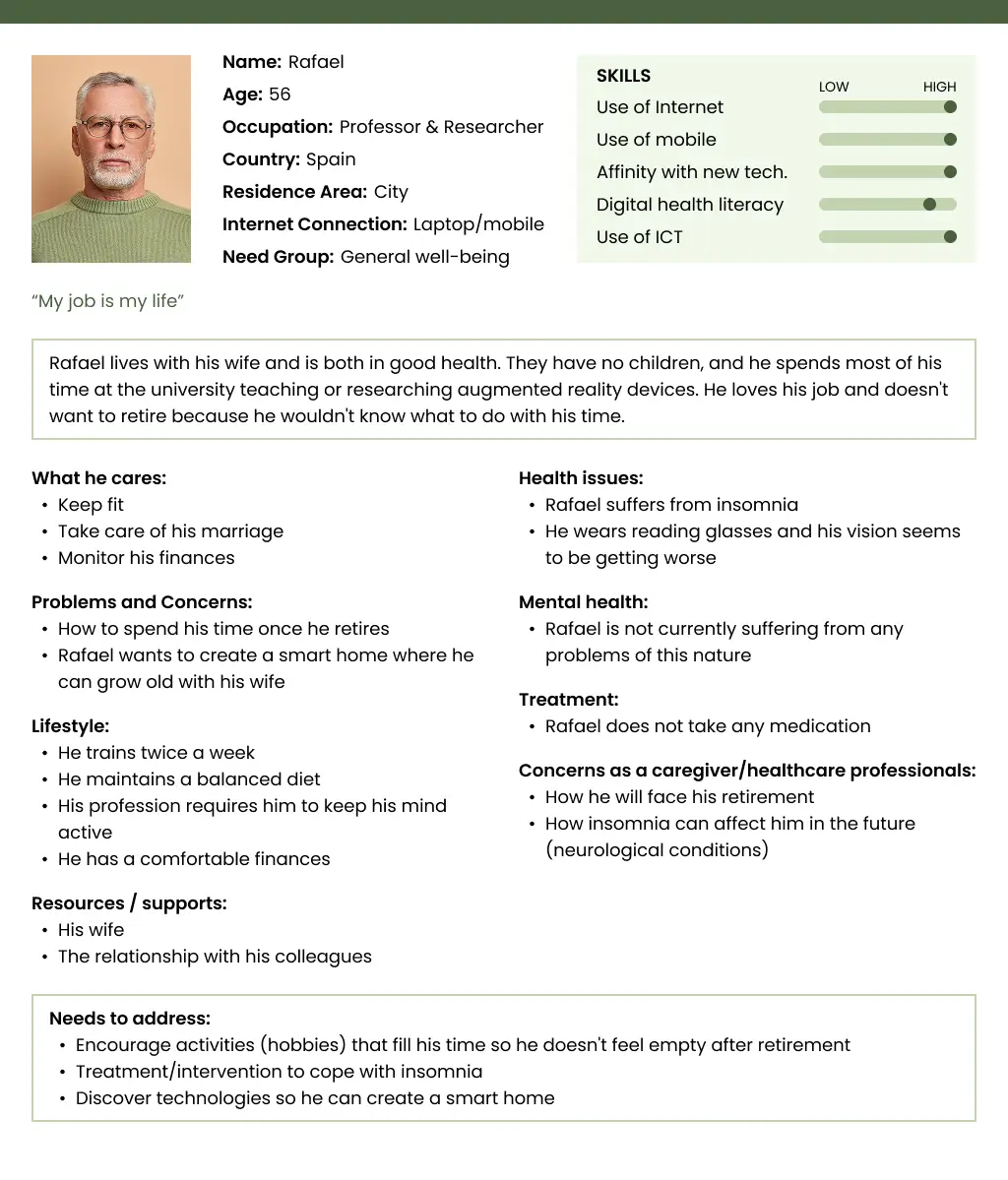
- Age is divided into: adults approaching retirement (55 and older), retirees under 75, an age group corresponding to the following decade (75-85 years), and finally, people over 85.
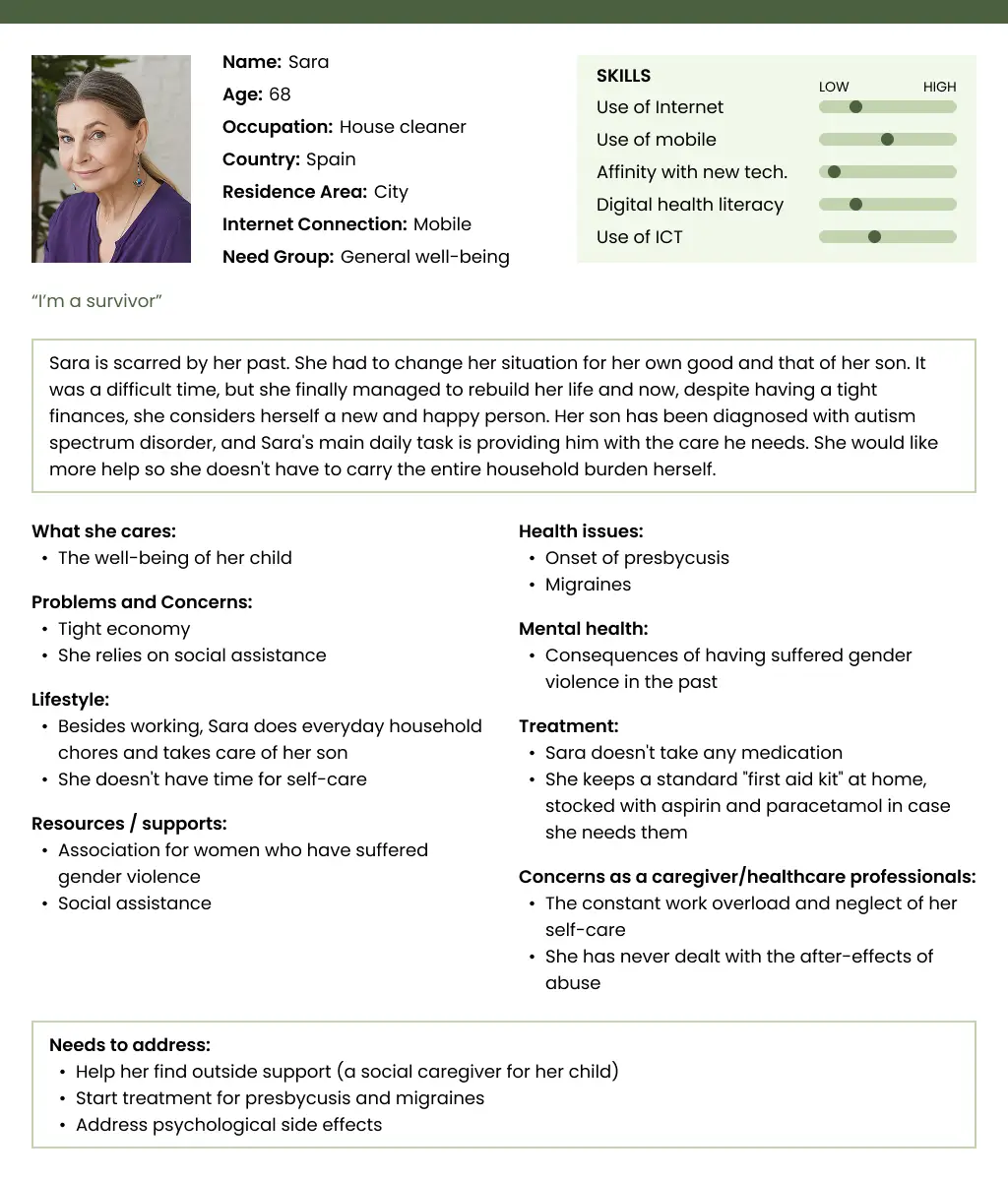
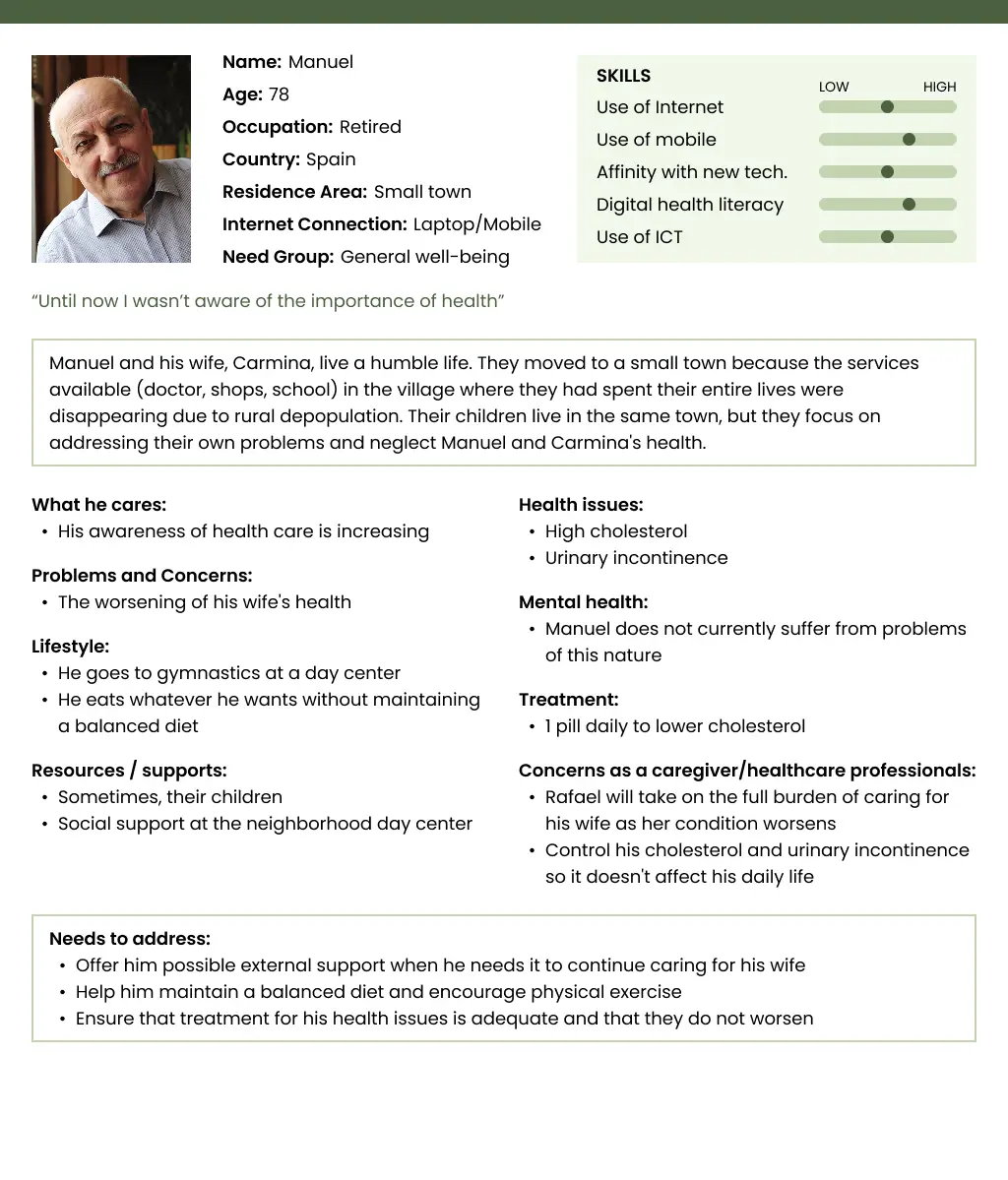
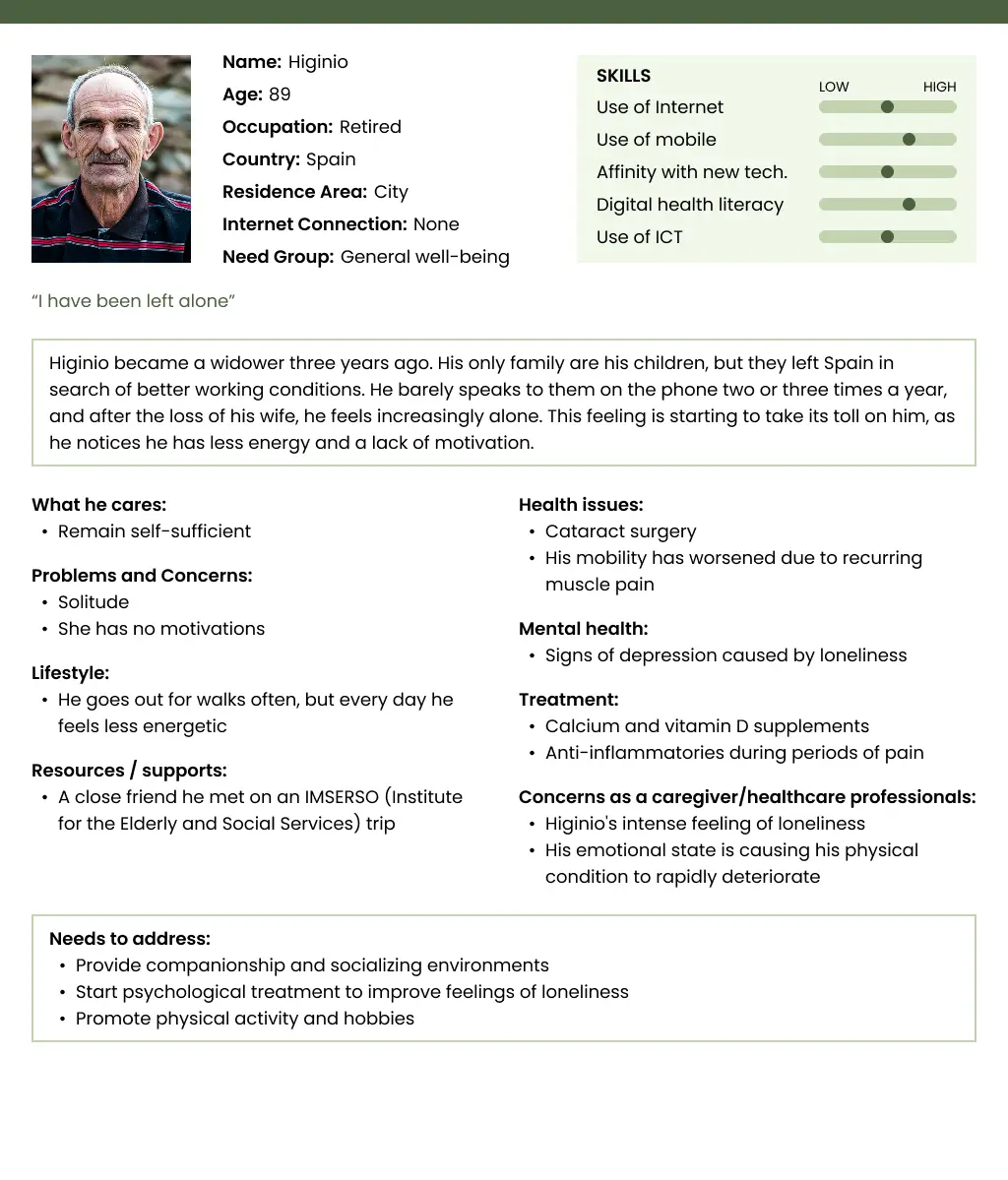
- The needs dimension gives rise to three groups: those with general well-being, those with chronic conditions or social needs, and those with more complex needs.
To better illustrate the diversity of potential users, a matrix was created combining age groups and levels of need. Each cell includes non-exhaustive examples designed to cover the widest possible range of cases. In building these examples, the following aspects were taken into account:
- General health issues
- Mental health
- Social and economic factors
- Lifestyle and associated risks
- Personality traits, including their relationship with technology
Needs / Age
55-65 years
Retirees under 75
75-85 years
85+ years
- Worsening vision
- Insomnia
- Exercises twice a week
- Is very good with technology due to his profession
- Doesn't want to retire
- Onset of presbycusis
- Migraines
- She suffered gender-based violence in the past
- Her child is dependent
- Due to family responsibilities, she neglect her own needs
- High cholesterol
- Worried about his wife's worsening condition (chronic kidney failure)
- Attends gymnastics at a day center
- Increasing concern for his health
- Cataract surgery
- Loneliness (widowed and family far away)
- Does well on his own
- Goes out for walks often
- Is afraid his health will worsen
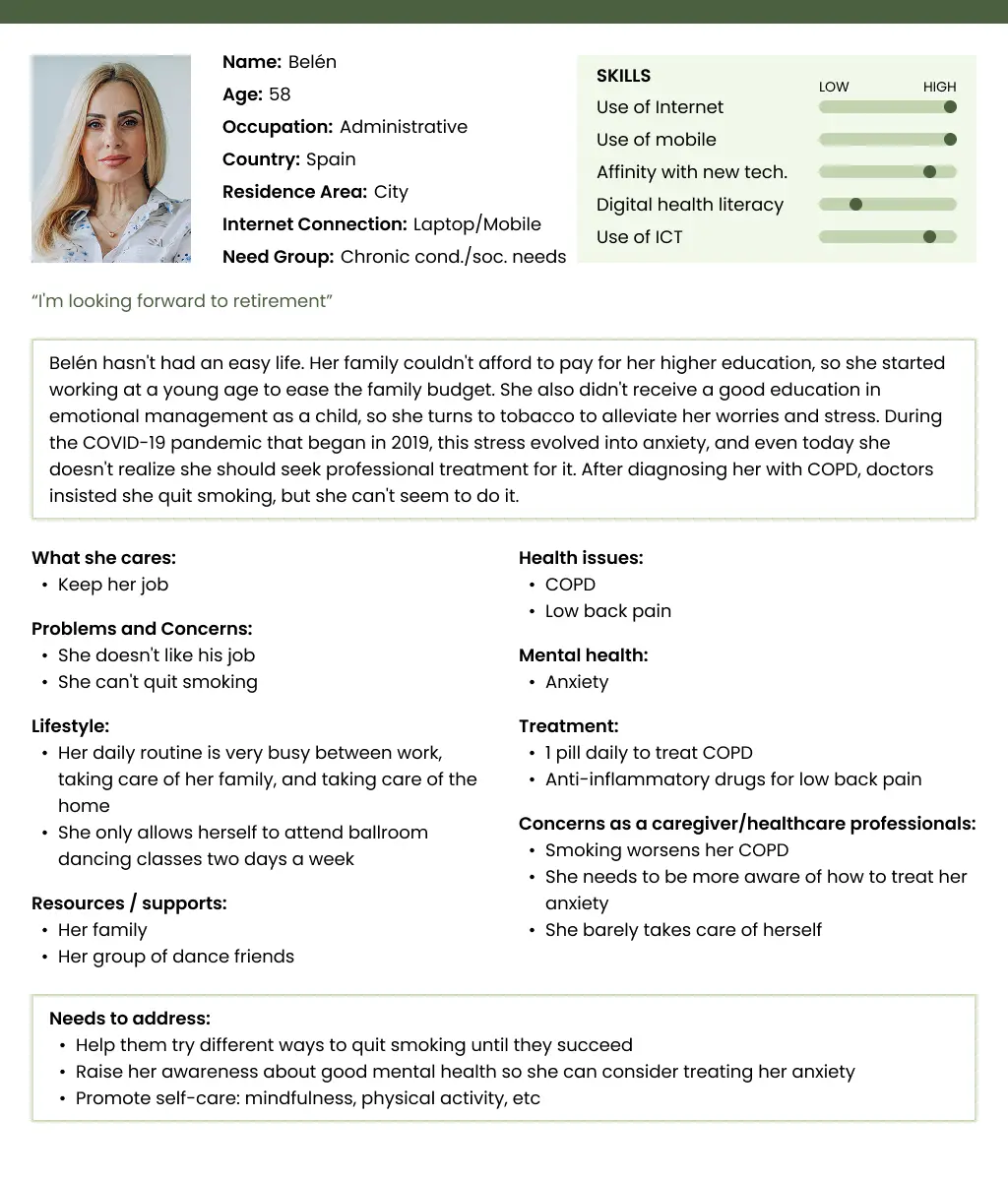
- With COPD and low back pain
- Anxiety due to COVID
- Doesn't like her job
- Can't quit smoking
- Used to technology because she works with a computer
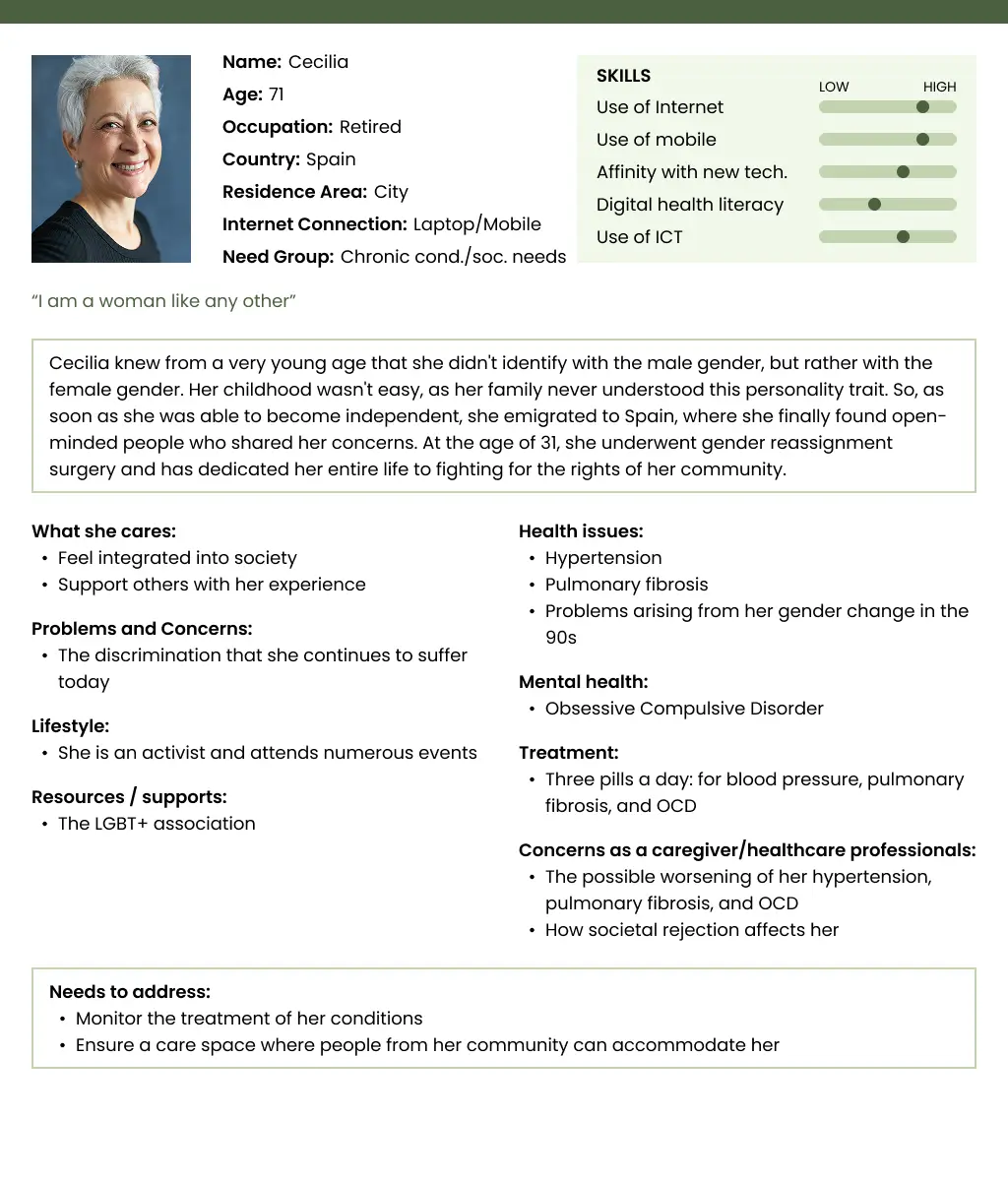
- Hypertension and pulmonary fibrosis (COVID-19 after effects)
- Obsessive-Compulsive Disorder (OCD)
- Poor family relationships
- She is an activist
- She changed her gender at 30
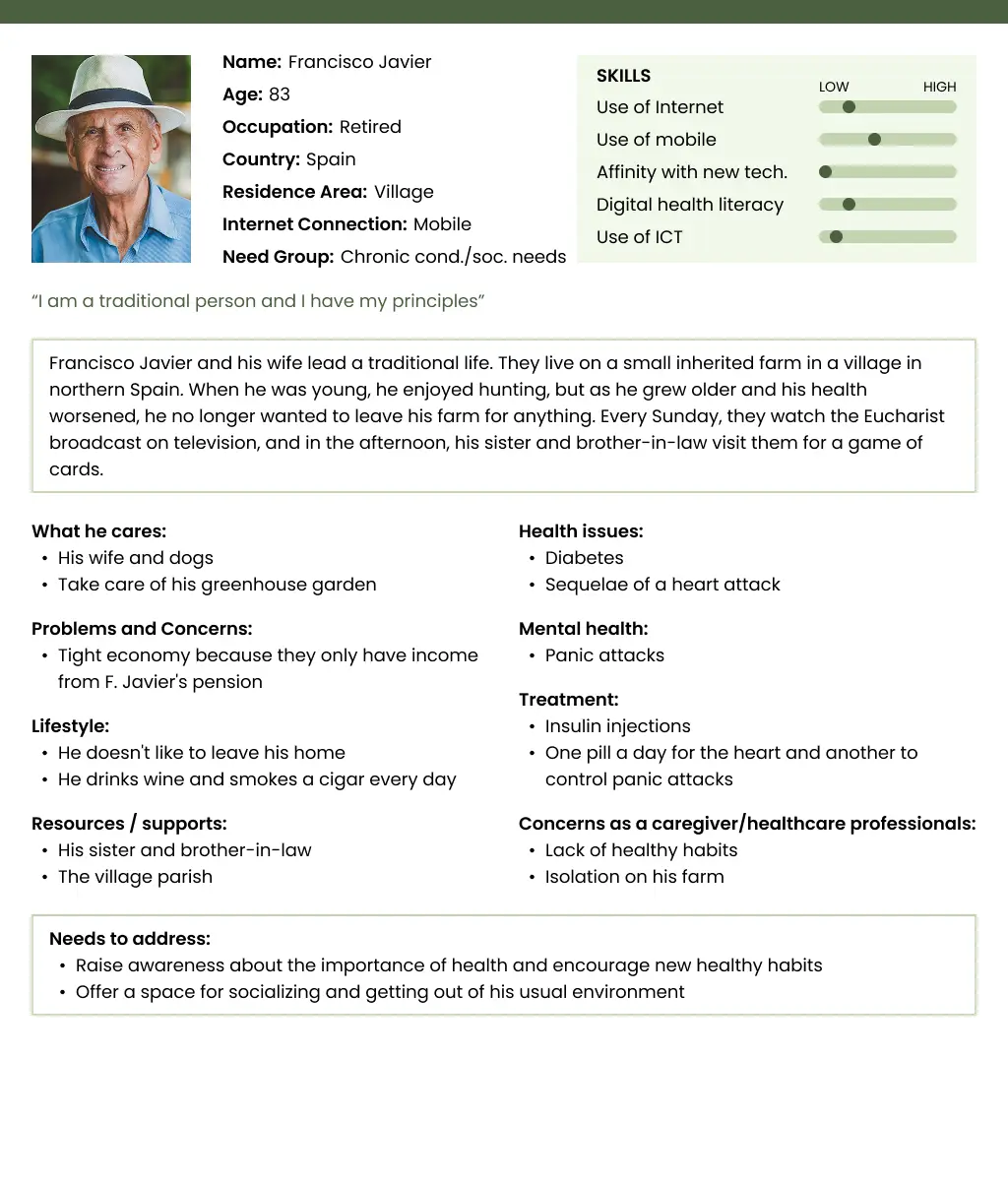
- Diabetes, after-effects of a heart attack
panic attacks - He and his wife live off their pension.
- He doesn't like to leave the house.
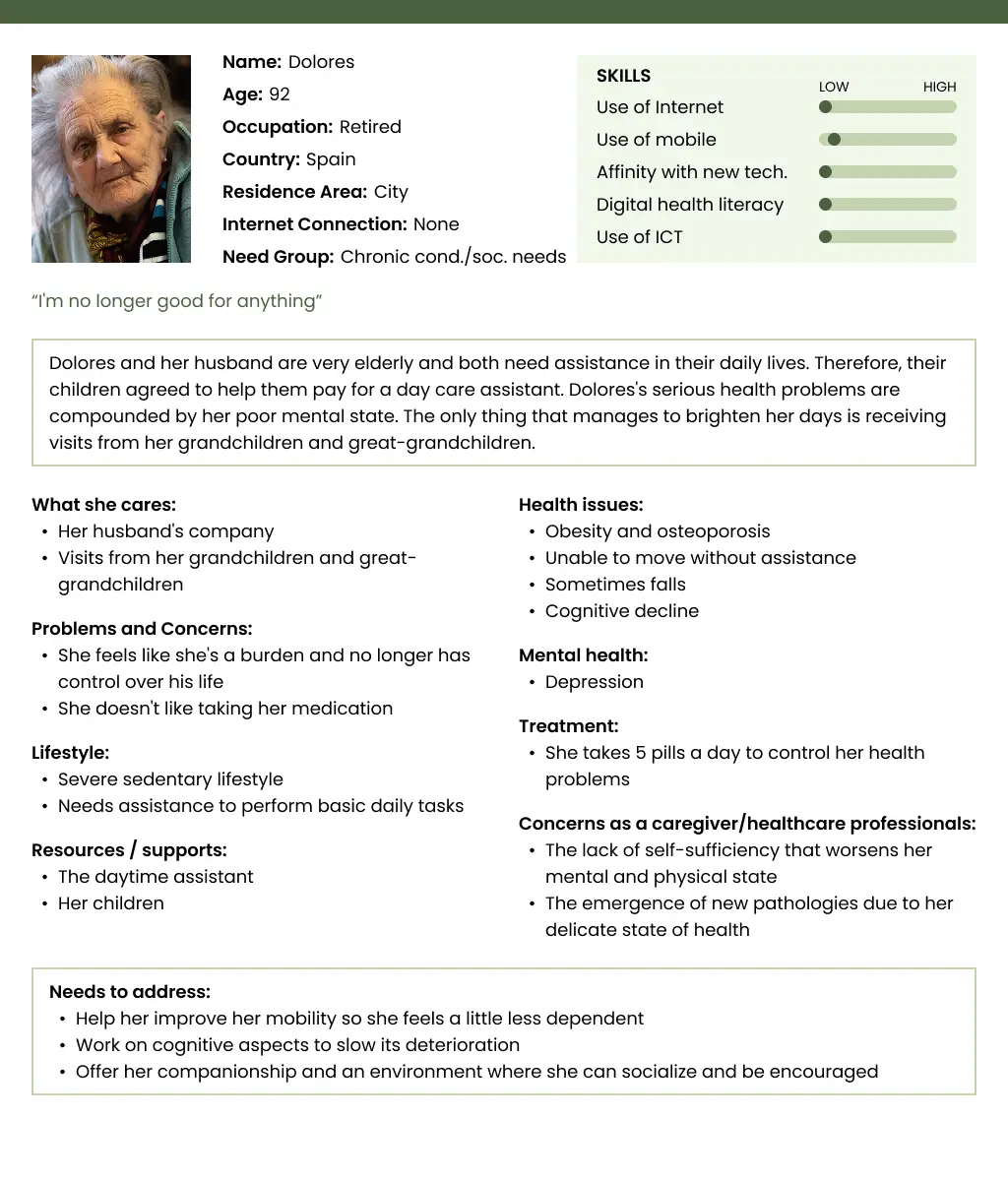
- Obesity and osteoporosis, falls, cognitive decline
- Depression
- Her husband can't care for her (she's elderly) so they have a daytime assistant
- Unable to move without assistance
- Glaucoma, paraplegia due to a traffic accident
- His wife helps him, but his strength is decreasing
- Financial problems
- Unhealthy diet because he eats due to anxiety
- He only uses technology to his advantage
- Prostate cancer
- Social phobia
- Divorced
- Has a poor relationship with his children
- Smokes and drinks heavily
- Refuses to accept outside help
- Parkinson's and early Alzheimer's
- She lives with her son's family, who cares for her
- She distrusts hospitals and healthcare professionals
- Rheumatoid arthritis, pacemaker, incontinence
- Advanced dementia
- His family visits her once a month
- She lives in a nursing home
Following the Blueprint of the EIP on AHA, I created 8 detailed personas as an extension of the stratification matrix. These personas were developed from the first two rows of the matrix (general well-being and chronic/social needs). Designing for the third row (older adults with complex needs) would have required a much more specialized approach, which was beyond the scope of this project.
Define
After mapping the context and user profiles, the focus of action was defined: a personalized interactive journey that allows visitors to the Smart House Living Lab to discover innovative health and well-being technologies in an engaging way.
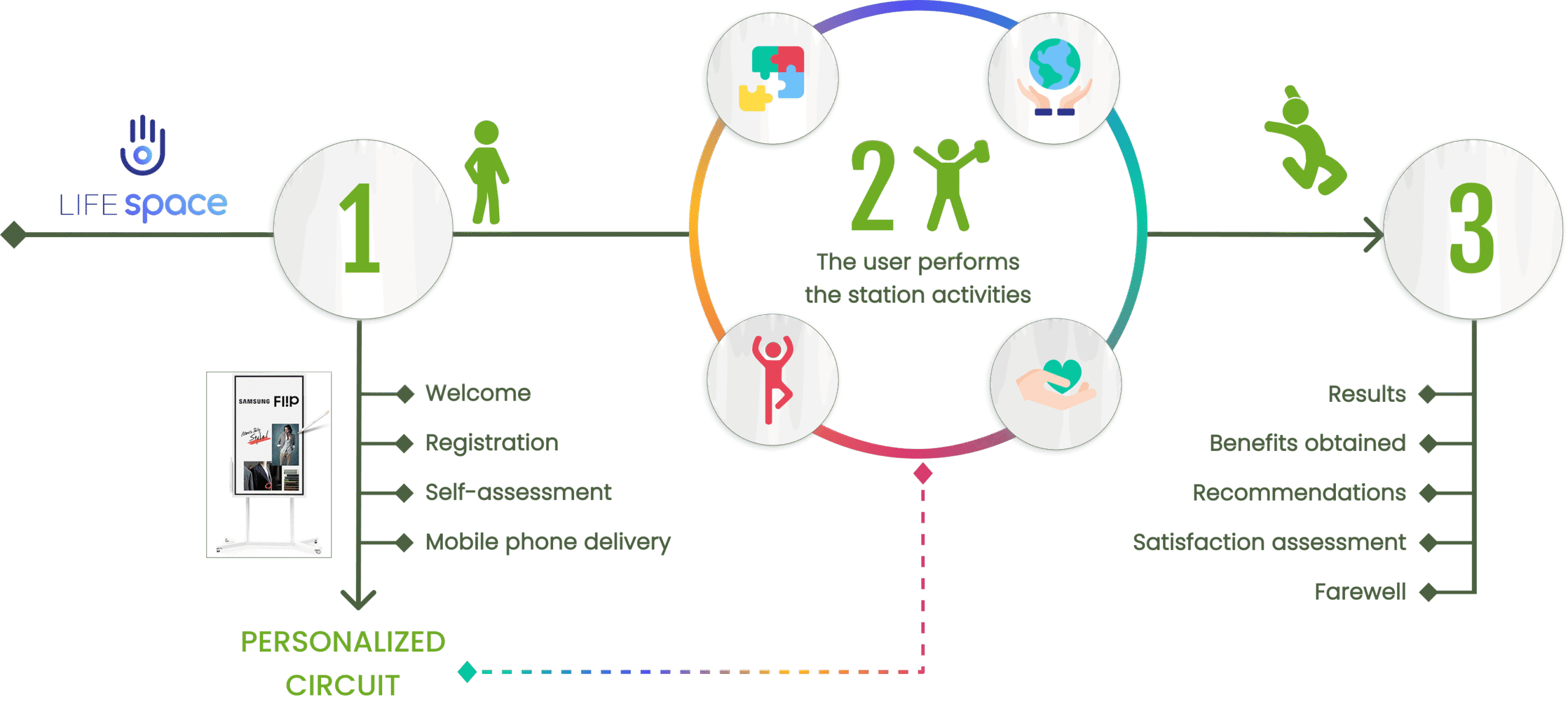
To make this concept tangible, I designed a user journey that any participant could experience inside the Living Lab:
- Welcome & Self-Assessment: Visitors are welcomed at digital screens, registered, and guided through a self-assessment. Based on their results, they receive a personalized activity circuit and a mobile phone to interact with the stations.
- Interactive Circuit: Users explore the Lab freely, moving between marked stations. At each one, the gadget triggers the activity, collects responses, and provides short feedback before suggesting the next step.
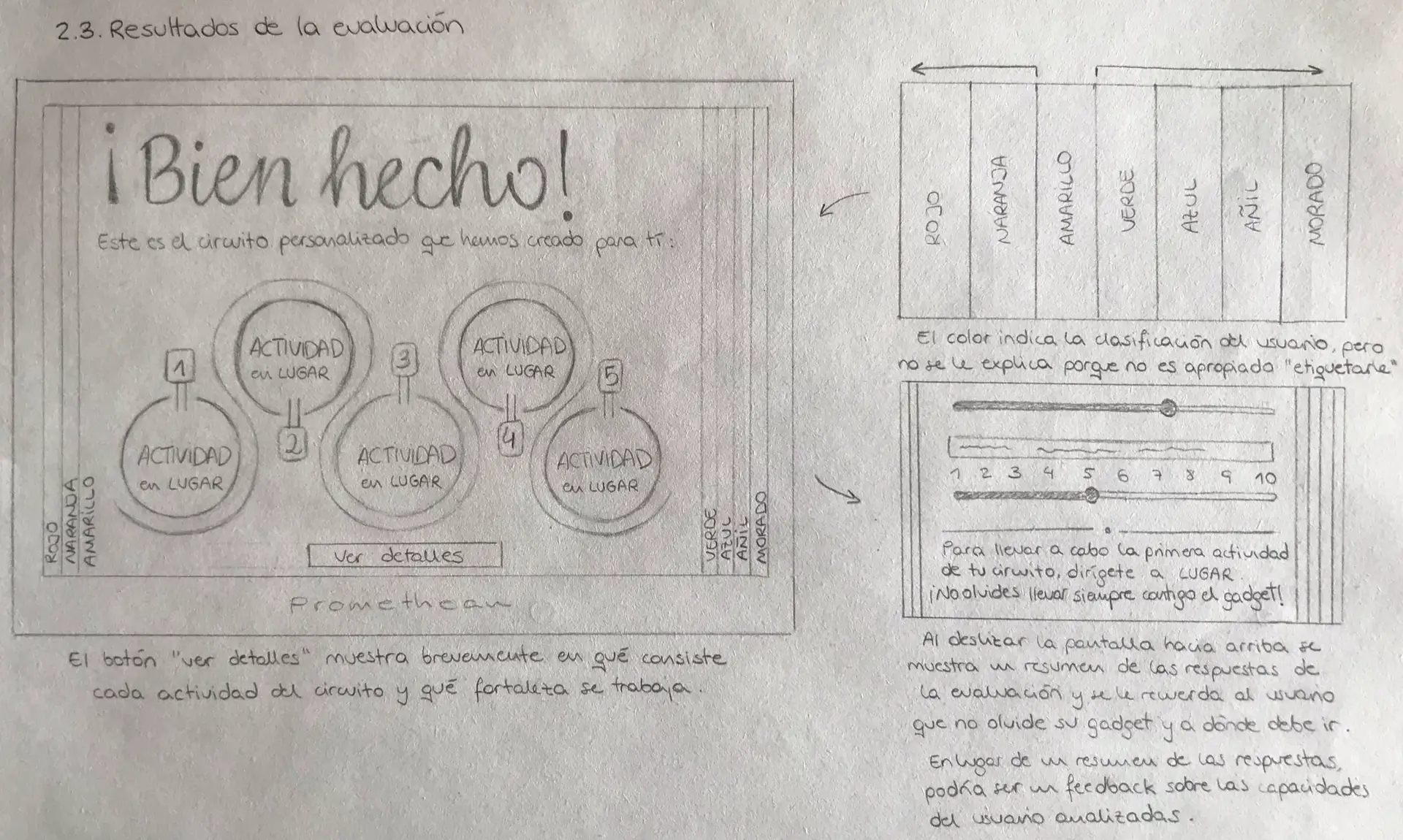
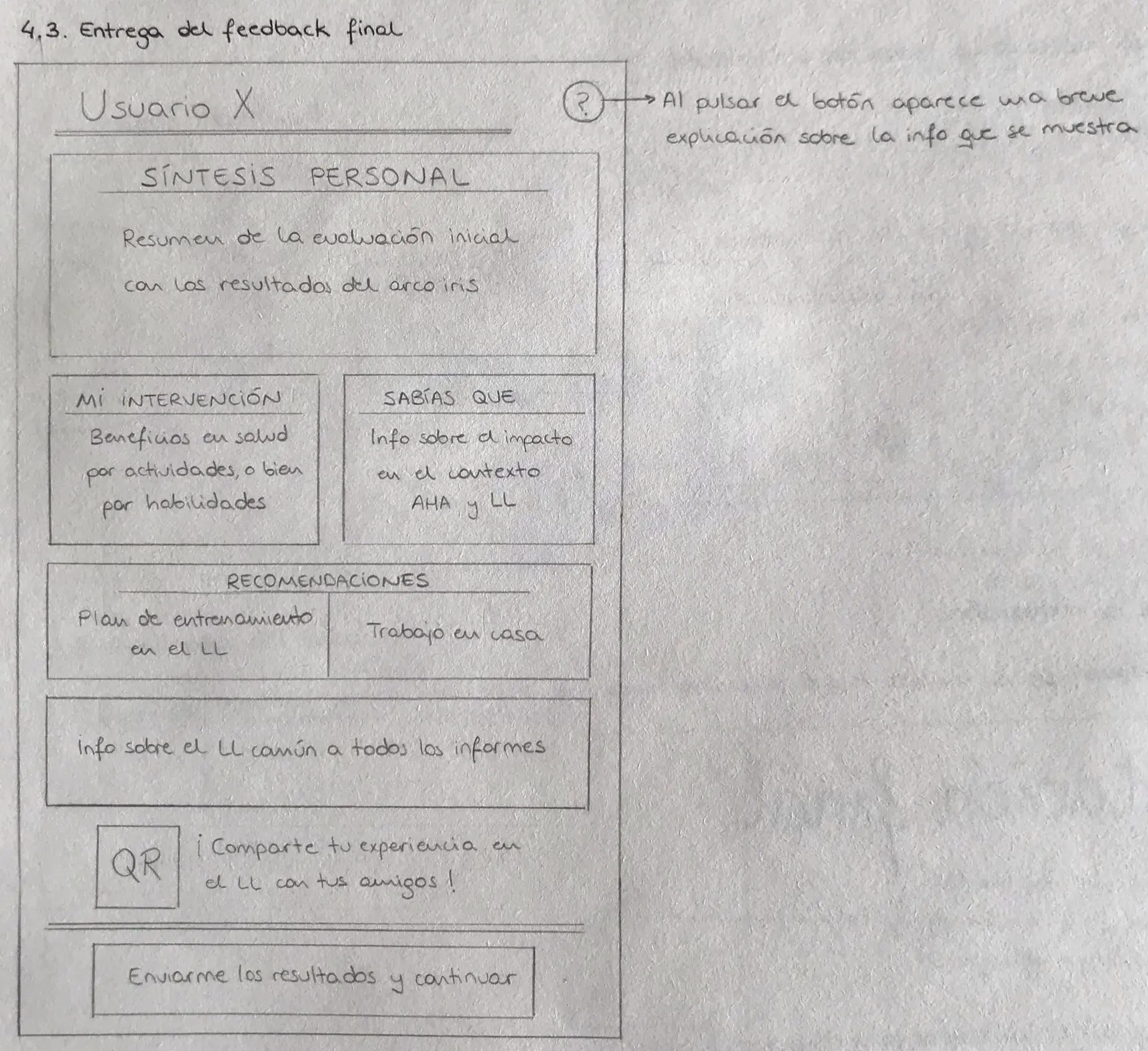
- Results & Recommendations: At the end, participants receive gamified results summarizing their performance, benefits obtained, and personalized recommendations for improving their health and well-being. The gadget is returned, and the visit closes with a short final evaluation.
To ensure scientific rigor, a protocol was developed in collaboration with LifeSTech researchers. It included:
Informed consent forms and user registration data.
Health self-assessment questions based on the validated Edmonton Frailty Scale.
Classification of users into four levels (Active, Normal, Frail, Dependent), aligned with the earlier Personas exercise.
Personalized activity circuits drawing from LifeSTech technologies in four categories: physical activity, cognition, lifestyle & well-being, and age-friendly environments.
Metrics and outcomes collected throughout the journey, provided back to the user as feedback.
Since the full protocol was too complex for regular visits, a “lite” version was created as the first iteration: shorter, easier to implement, and still impactful. This prototype acted as a mold for future versions, balancing innovation with feasibility.
Design
The design process moved through both low-fidelity sketching and high-fidelity prototyping, each serving a different but complementary purpose in shaping the final interactive experience.
LOW-FIDELITY PROTOTYPE
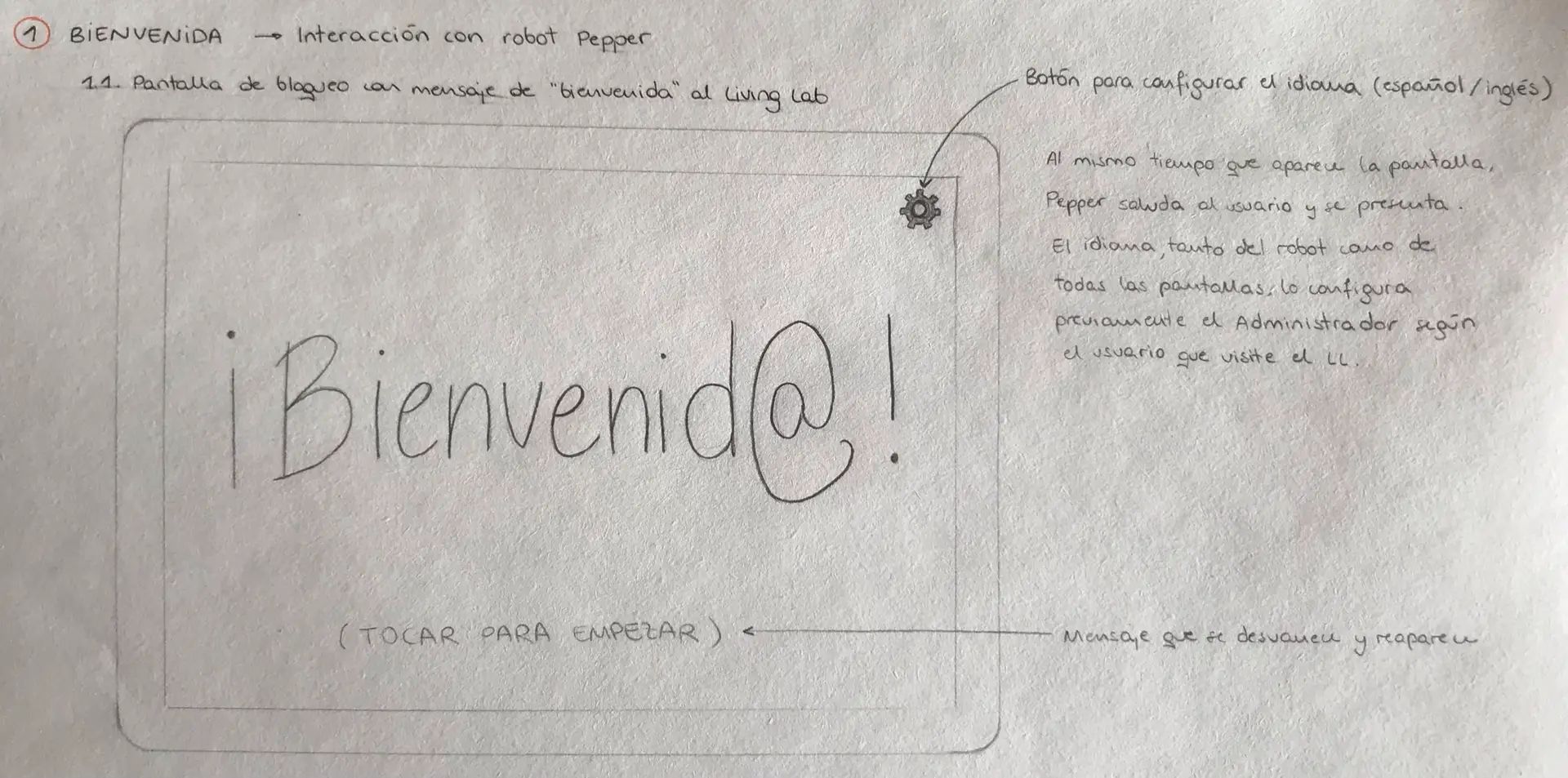
The first prototypes were created by hand. At this stage, the goal was not polish, but alignment: giving all stakeholders a shared vision of how the journey could unfold.

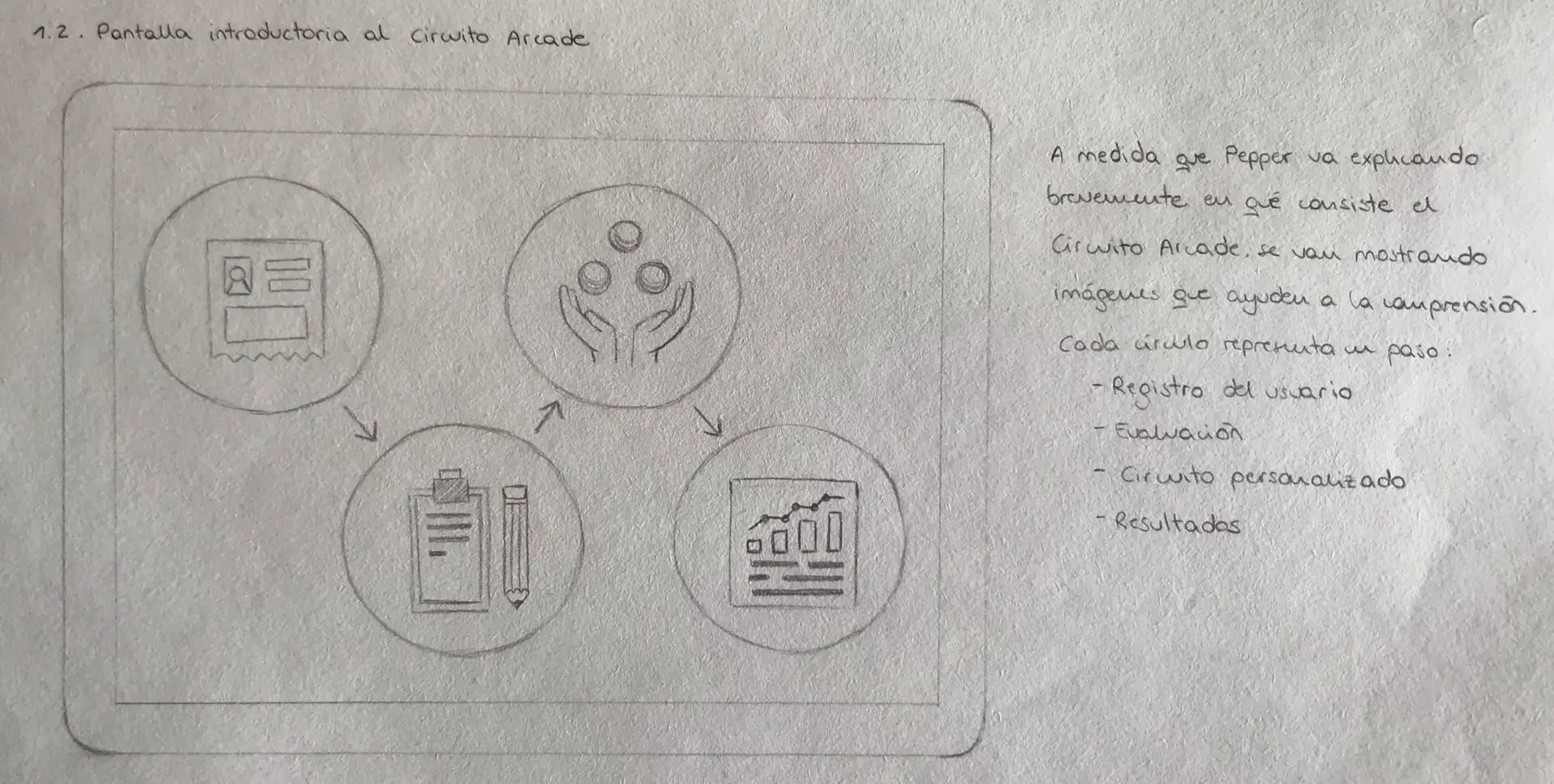
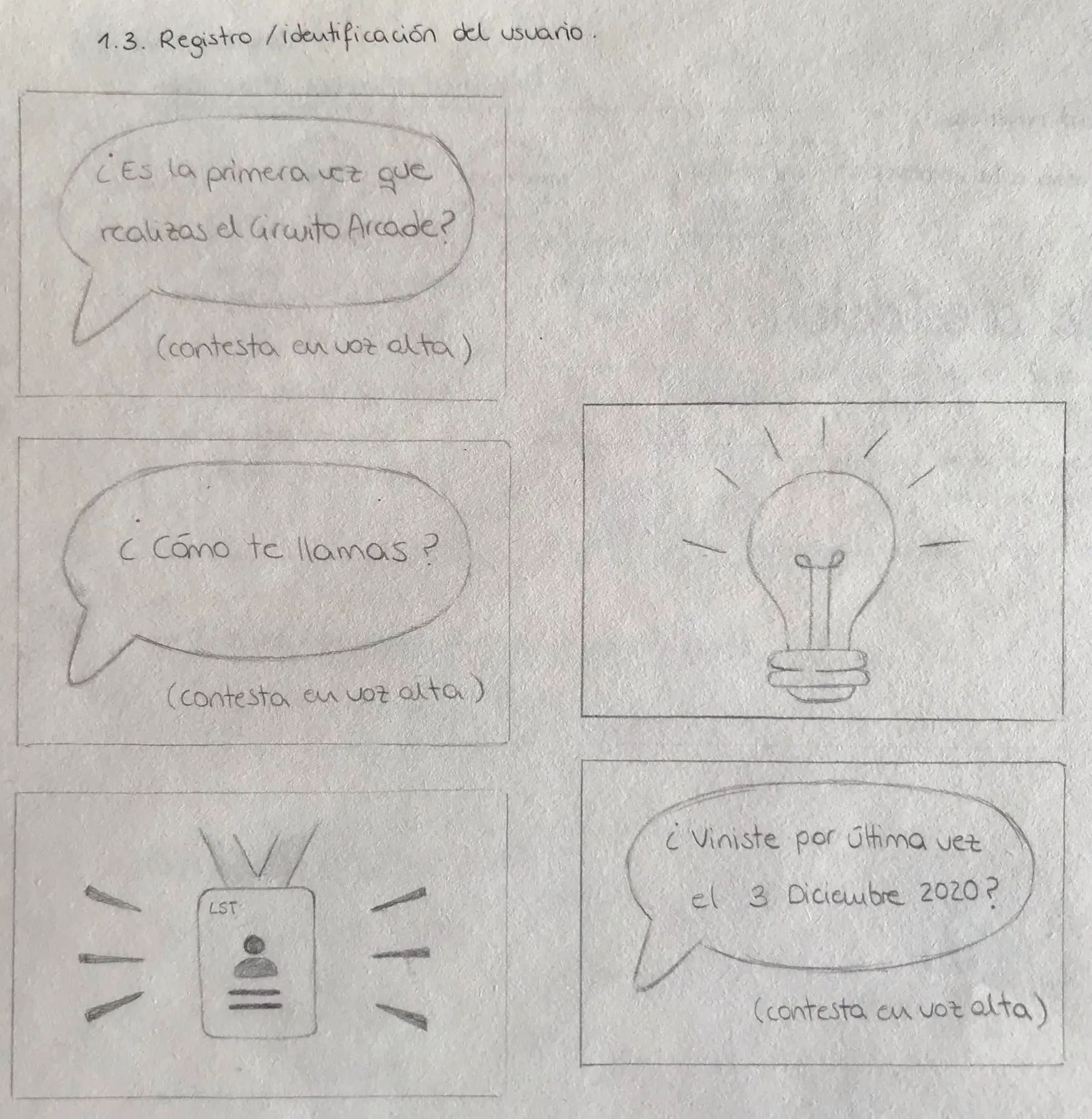
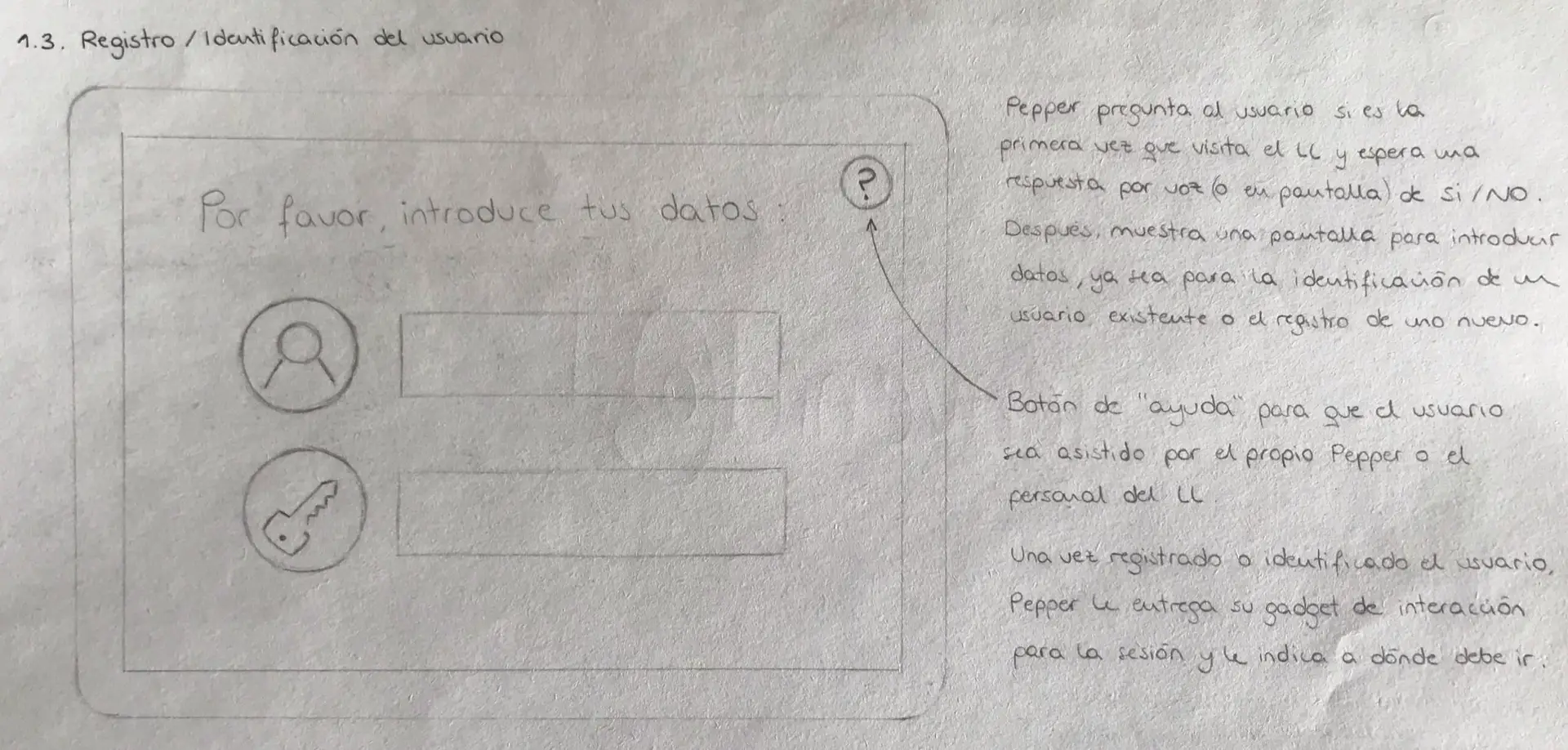
An early proposal envisioned welcoming users through Pepper, the humanoid robot, with a conversational interface supported by simple visual prompts on its chest screen. These sketches illustrated Pepper’s role in guiding users through the opening interaction, while the main self-assessment and navigation screens were designed for a large horizontal display (e.g., Promethean interactive screen).
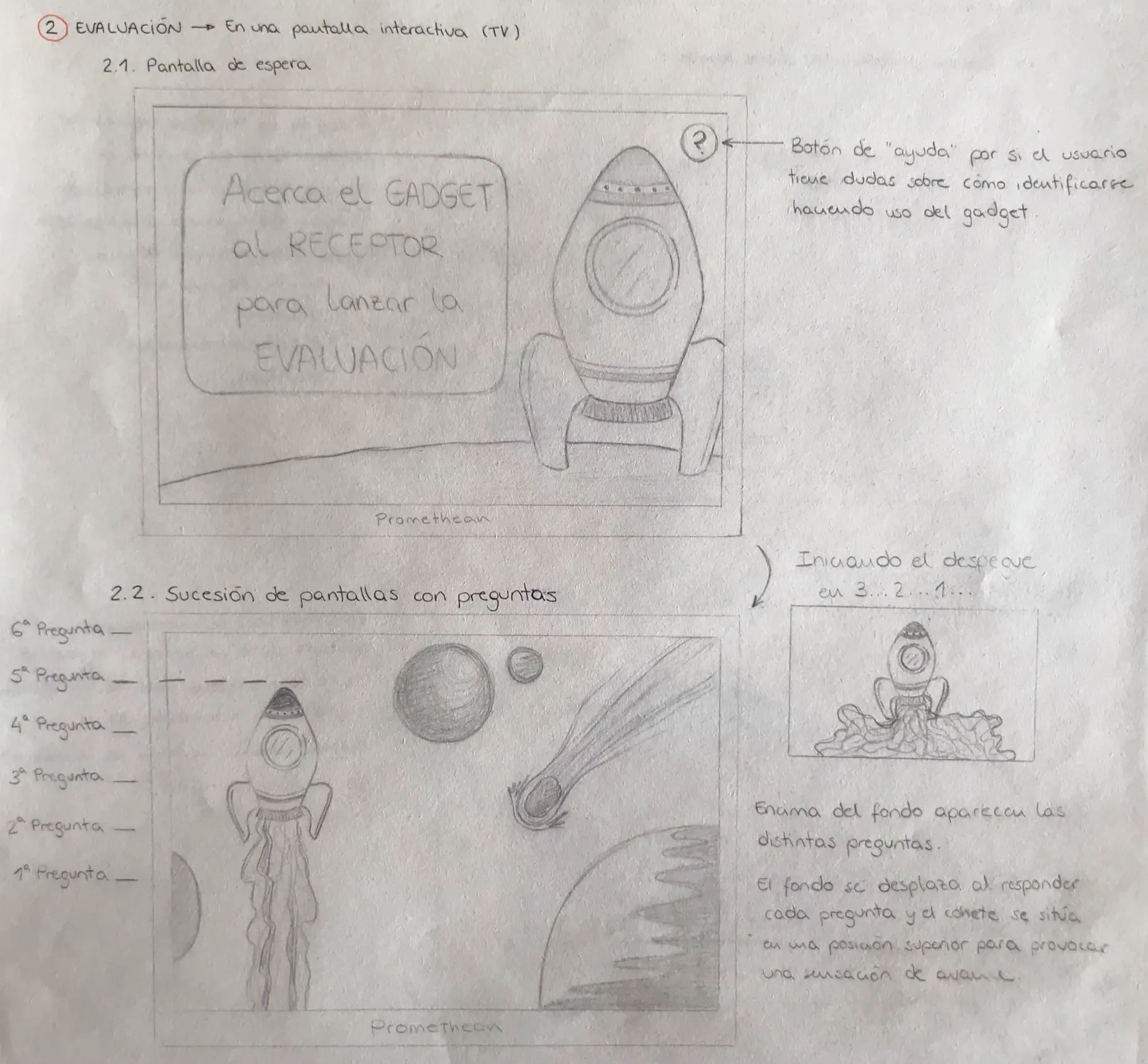
To make the experience more engaging, I also proposed a space-themed journey, where each activity was envisioned as a “space station” within the circuit.
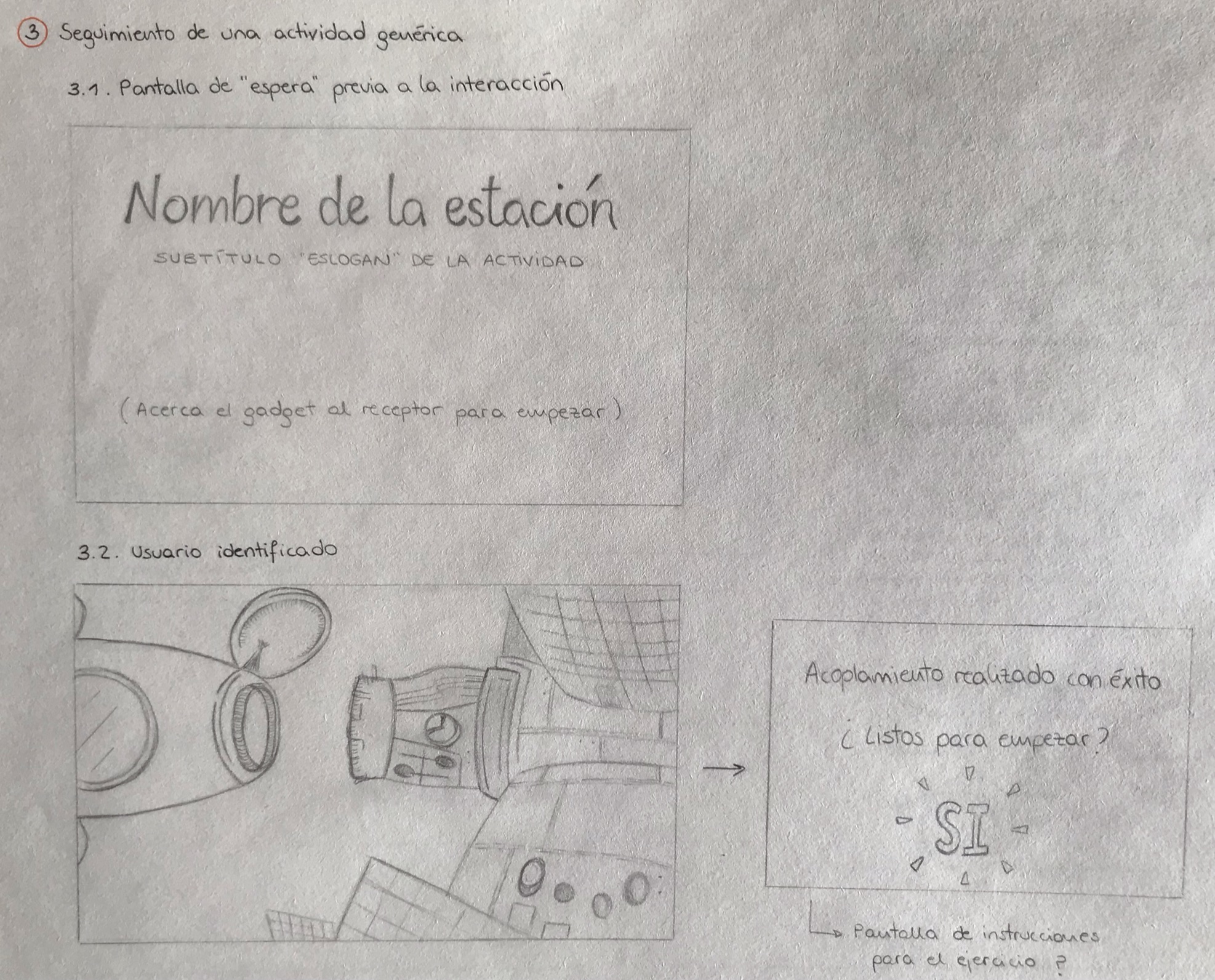
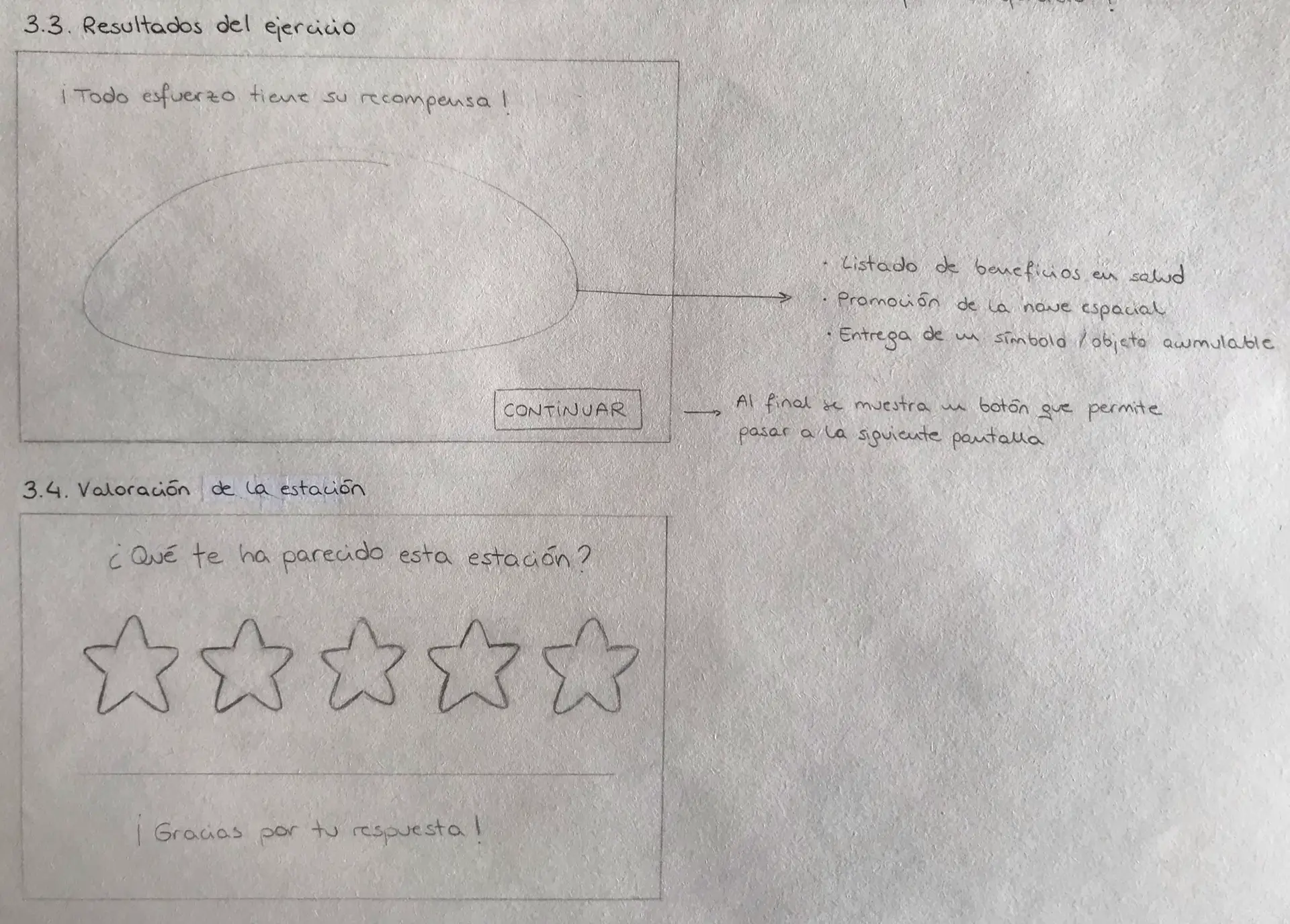
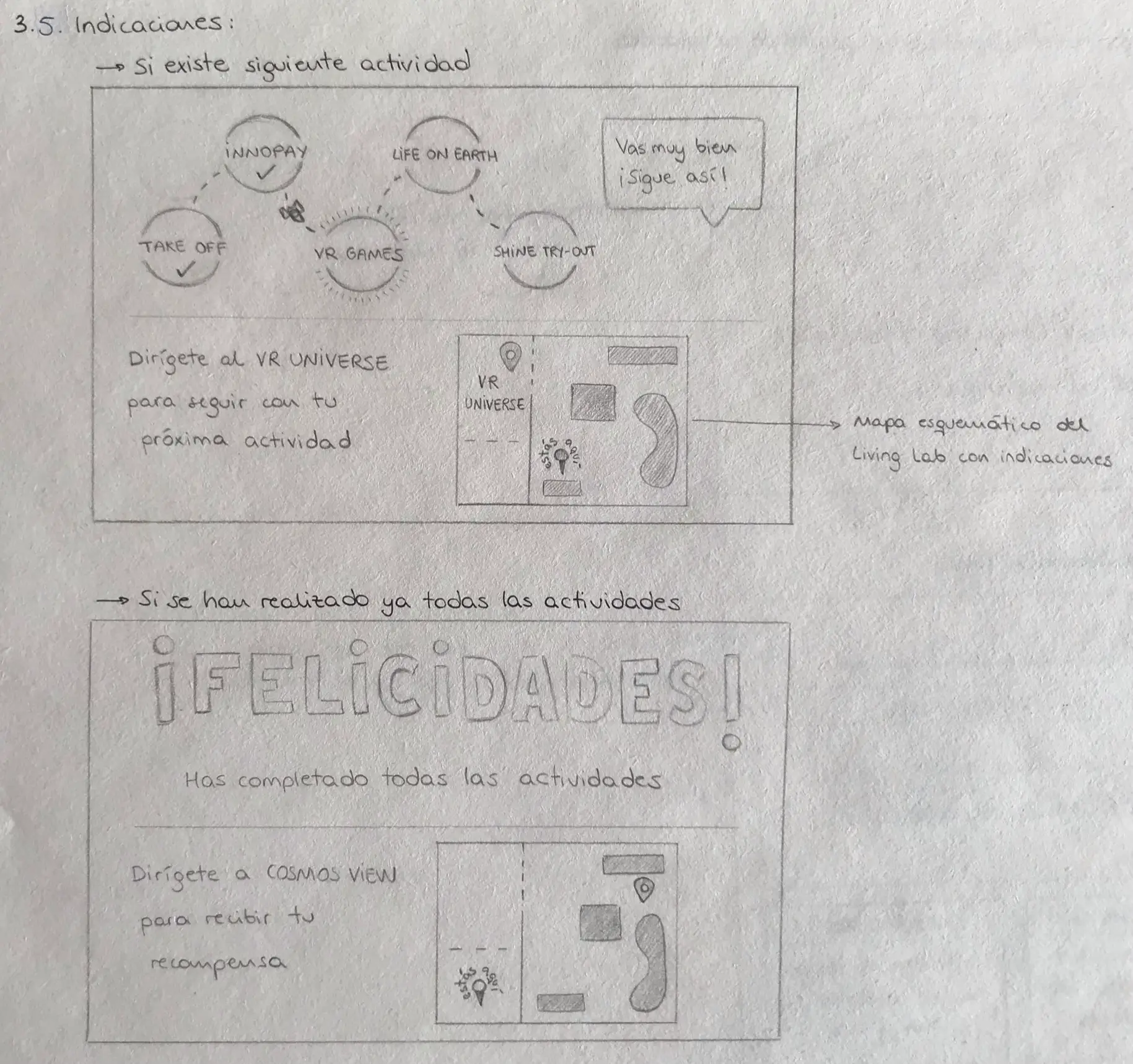
While these sketches had little resemblance to the final design, they were invaluable in sparking discussion and steering the multidisciplinary team toward a common direction.
HIGH-FIDELITY PROTOTYPE
Once the protocol and technological integration matured, I created high-fidelity prototypes in Figma, refined through multiple iterations and testing sessions. The final interactive flow was designed across two devices:
Samsung Flip
Used for the welcome, register, self-assessment, and personalized circuit assignment.
Mobile phone
Provided a quick guide for the circuit activities, recording progress, and visualizing results and advices.
Testing
Because of the COVID-19 context, organizing an in-person validation with older adults was neither safe nor realistic at this stage. Instead, I conducted a heuristic evaluation with five usability experts from LifeSTech, all with extensive experience designing and testing health and AHA solutions.
The process followed Nielsen’s principles and unfolded in two phases:
- Each evaluator independently reviewed the prototype and reported usability issues, rating their severity based on frequency, impact, and persistence.
- Findings were then cross-shared so evaluators could refine severity scores collectively.
This approach surfaced a range of design refinements, including:
- Writing “ESPAÑOL” and “ENGLISH” in full on the welcome screen (avoiding abbreviations).
- Adding a “back to start” option during user registration.
- Rewriting unclear consent form text.
- Improving progress indicators so they showed completed steps rather than just the current one.
- Clarifying instructions after each activity and at the end of the circuit.
- Replacing technical jargon with plain language (e.g., “modules” → “activities”).
Although this method lacked the direct input of elderly participants, it provided valuable expert feedback to refine navigation, clarity, and accessibility. The results shaped the final high-fidelity prototype, ensuring it was closer to being ready for a real-world pilot.
Next steps
As with any realistic innovation, advancing this prototype requires the coordinated effort of a multidisciplinary team (designers, developers, researchers, and healthcare professionals) working together to integrate technology and refine the protocol.
Future steps could include:
-
Expanding the current “lite” version into a “full” experience with richer data collection and more precise user stratification.
-
Validating the solution with real users through scenario-based sessions, repeating refinement cycles until satisfaction goals are met.
-
Extending deployment beyond the Living Lab into everyday community settings, such as day centers or libraries, where older adults could benefit directly.
-
Designing tailored journeys for the other stakeholder groups (health professionals, companies/investors, students), ensuring that every visitor to LifeSpace finds a relevant, engaging use case.
Impact
Conference Highlight
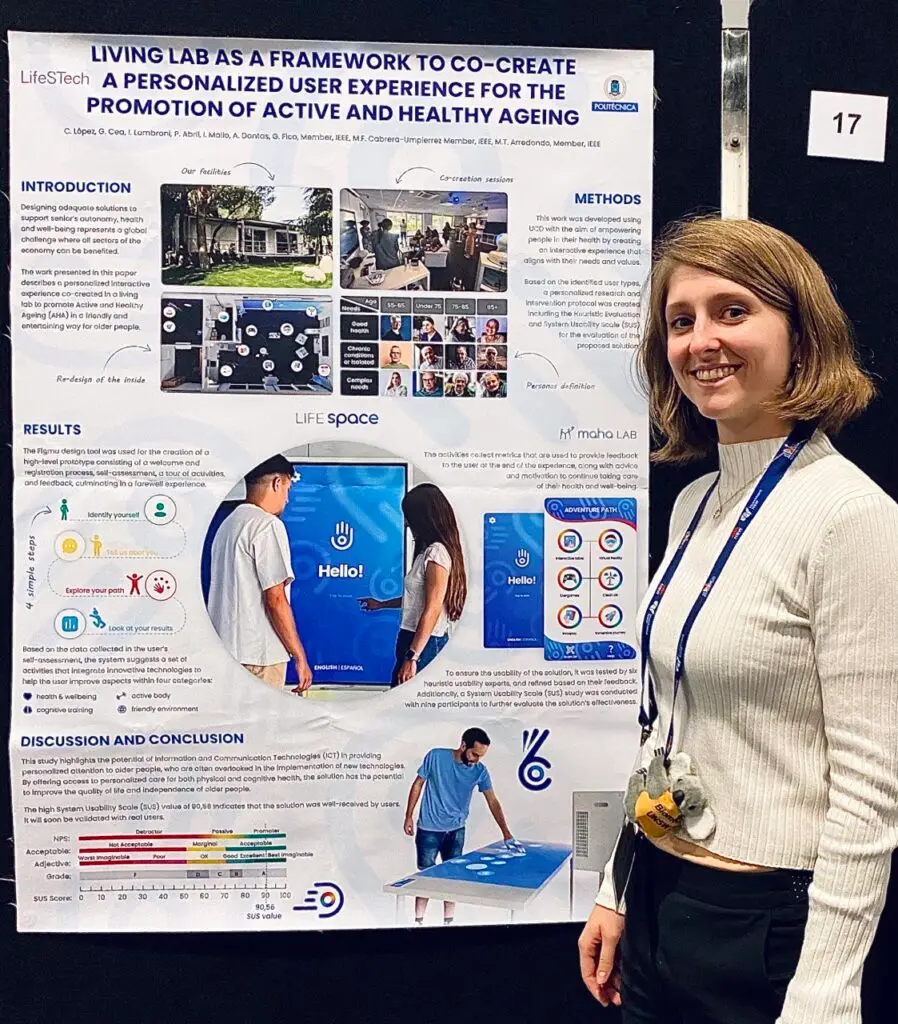
I was the first author of a 1-page paper that was accepted for IEEE EMBC 2023 in Sydney, Australia. I personally prepared the poster and presented it at the conference. Additionally, the prototype evaluation was updated using the latest SUS usability scores to provide current insights.
Showcase at the Living Lab
Although the solution has not yet been technically implemented in the Living Lab, the prototype has become a key demonstration asset.
During visits from ministries, universities, healthcare professionals, international collaborators, and even Princess Sofia, I guide visitors through the interactive journey using a Samsung Flip and a mobile phone, effectively illustrating LifeSTech research line on Active and Healthy Aging.

Reflection
This project marked my first real experience as a UX/UI designer in a multidisciplinary team. I learned how essential collaboration is when engineers, researchers, and designers must align around a shared vision. It taught me to listen actively, adapt my designs to different perspectives, and balance individual initiative with collective contributions.
I also discovered how challenging it can be to apply User-Centered Design in a real innovation environment. I learned to translate user profiles into personalized, gamified journeys while keeping healthcare rigor at the core. The heuristic evaluation showed me how even small details (like the clarity of labels) can significantly impact accessibility, especially for older adults.
Flexibility was another key lesson: progressing with limited stakeholder input, adapting to pandemic restrictions, and finding creative ways to keep momentum despite constraints. These challenges strengthened my ability to design solutions that balance scientific accuracy, engaging interaction, and real-world feasibility.
Finally, I would like to thank my Final Degree Project (TFG) supervisors Ivana Lombroni, Gloria Cea, and Giuseppe Fico, who encouraged me to find a creative voice within engineering. I am also grateful to Adrián Dantas and Irene Mallo, who contributed significantly to shaping the visual identity of LifeSpace and with whom I shared valuable design work and perspectives throughout this process.